Written by Thomas Lane, NCPS, CRPS
What’s in a word? Much more than many of us realize.
In the context of behavioral health, substance use and even physical health challenges, using terms and phrases that group people by diagnosis, disability, disease and other characteristics perpetuates stigma, discrimination and exclusion. Yet this type of language has been part of the healthcare lexicon for decades. Outdated terms such as “addict,” “crazy” or “diabetic” are just a few common examples.
We live in a time when individuals are at the center of the healthcare field. As healthcare consumers, individuals are empowered to make their own health choices. As healthcare professionals and activists, we need to mirror this empowerment, and seize the opportunity to pivot how we portray what we do. We need to move away from archaic language that contradicts all of the positive changes we help individuals make in their lives on a daily basis.
This is where “person-first language” can make a big difference.
What is person-first language?
Person-first language means seeing people as “people first,” and not as their disease, illness or disability, or as part of a homogeneous group. It portrays individuals living with behavioral health, substance use or physical health challenges beyond a lens of illness, diagnosis and hopelessness. It helps address issues relating to illness-identity and self-stigma, keeping in mind that we are all unique individuals, with unique lived experiences.
At Magellan Health, our use of person-first language stems from our work in behavioral health, but it applies to everything we do with equal emphasis. It shows our commitment to being culturally and linguistically appropriate in all of our communications. It models our principles of recovery and resiliency, and contributes to evolving and improving our organizational culture.
On a personal level, as an individual in recovery myself I can tell you how important person-first language became to me as I discovered the often unintended consequences of using language that robs one of their individuality. We all deserve respect and appreciation for our unique qualities.
How is person-first language used?
Using person-first language is an intentional practice. Here are some examples of old language that is commonly used in comparison to newer, person-centered language that can be applied by anyone:
- From “chronic disease management” to “improving health outcomes for people living with chronic health conditions.”
- From “illness self-management” to “improving health education, support and community inclusion to promote individual wellness and self-direction.”
- From “crazy, nuts, lunatic” to “someone who may benefit from services and supports.”
- From “individuals suffering with a mental illness” to “individuals with a mental illness.”
For practice, try to recognize when others use the outdated or inappropriate terms and phrases above. And ask yourself how often you use them. Then, make the conscious choice to omit them from your vocabulary and replace them with new terms. While changing an old habit can be a challenge, consciously developing a new one is an easier path to meaningful change.
Remember, we all have choices about the words we speak and write. Those choices can either affirm the distinctive individuals that we are — or diminish us with labels. The words we use can fill us with hope, or burden us with despair. So let’s choose hope.
Changing the way you speak and write is a gradual process. But by putting the person first when you do, you can play a role in bringing our healthcare language into the 21st century.
For more information and resources, please visit Magellan’s e-Learning Center: http://www.magellanhealth.com/training-site/home.aspx
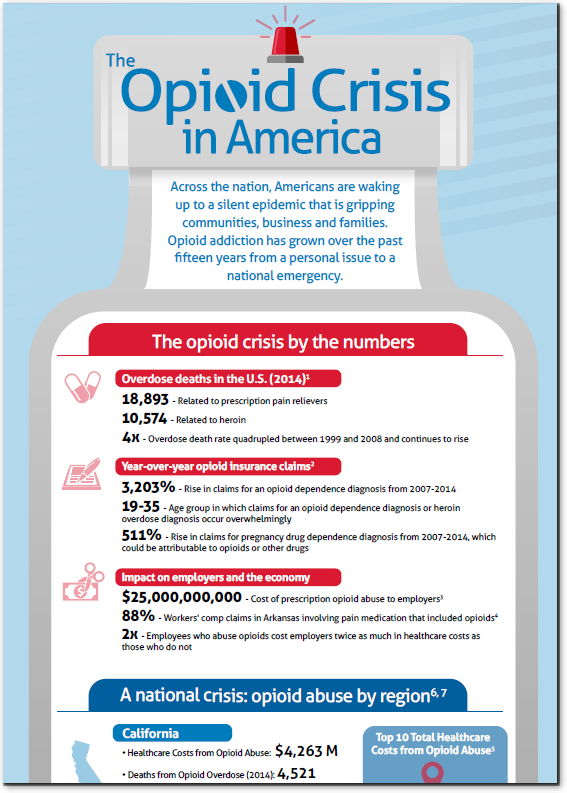
 Dr. Shareh Ghani, vice president medical director at Magellan Healthcare, and lead author of the study spoke of the importance of fully understanding the scope of the addiction crisis: “Having worked in commercial and Medicaid markets, I have reviewed numerous cases of accidental overdose and suicides related to pain prescriptions. The opioid crisis in this country demands that we understand the issue and identify predictors of risk.”
Dr. Shareh Ghani, vice president medical director at Magellan Healthcare, and lead author of the study spoke of the importance of fully understanding the scope of the addiction crisis: “Having worked in commercial and Medicaid markets, I have reviewed numerous cases of accidental overdose and suicides related to pain prescriptions. The opioid crisis in this country demands that we understand the issue and identify predictors of risk.”