From Compassion To Action: Not Staying Silent on the Silent Epidemic
The following is an excerpt from the 2018 Magellan Community Impact Report.
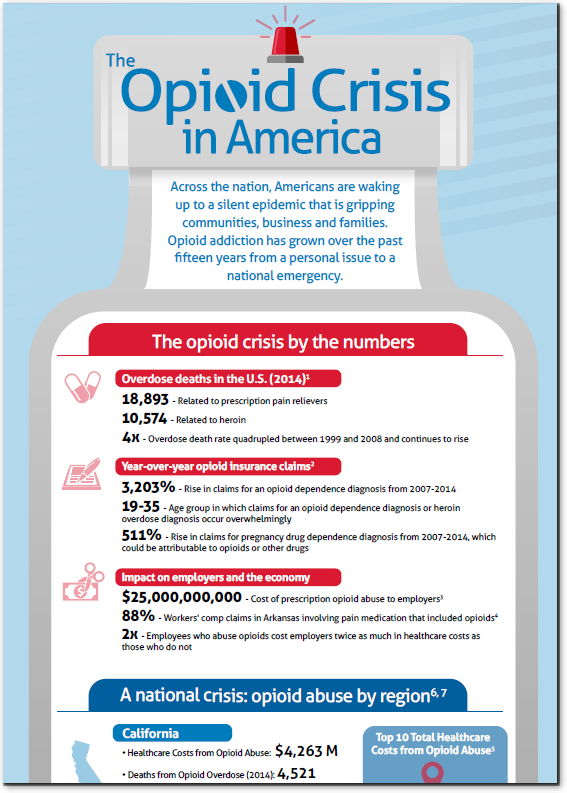
It is estimated that 130 Americans die every day from an opioid overdose. The opioid epidemic has become a national crisis and is continuing to grow rapidly, affecting families in every city across our nation.
No one is exempt from experiencing the effects of the opioid crisis. Magellan’s own Janet Edwards, RN, senior clinical director of Magellan’s Chronic Pain Management program, describes how close to home the opioid epidemic hit her:
It is estimated that 130 Americans die every day from an opioid overdose. The opioid epidemic has become a national crisis and is continuing to grow rapidly, affecting families in every city across our nation.
“My daughter, Nikki, was 26 when she died of a Fentanyl overdose. As the mother of a six-year-old and a critical care nurse working in a respected healthcare organization, Nikki was the picture of success. But to handle the pressures of nursing school, a full-time job, and life as a single mother, Nikki sought prescriptions for Adderall and Xanax from multiple physicians. Over time, her addiction to these substances gave way to a new addiction: Fentanyl, which she began to confiscate from the critical care unit where she worked.
Like many others, Nikki didn’t show any signs of addiction. But five years after her son was born, Nikki sat at my kitchen table and admitted that she was addicted to heroin. She was afraid to get help, because she did not want to lose her job or the respect of her peers. She insisted she could recover on her own. Even though I, as a nurse, knew the odds were not good that Nikki could manage her recovery alone, I respected my daughter’s wishes. It’s a decision I will forever regret. Eleven months later, Nikki died of an accidental overdose in front of her son and a friend.”
Following the loss of her daughter, Janet has openly shared Nikki’s story, becoming an advocate for helping prevent opioid addiction. Further, Janet has taken on clinical leadership of Magellan’s Chronic Pain program, which offers alternatives to opioid use.
Meeting opioid users where they are
No matter where or how someone encounters opioids or where they may be in the cycle of use, dependence or addiction, Magellan offers many other ways to address the opioid problem. Our behavioral health products forged from decades of serving the public, our specialty healthcare solutions supported by clinical excellence, and our customized pharmacy programs are ready to answer the call as organizations and individuals look for answers.
Hosting a forum for sharing successes and discussing solutions
In September 2018, Magellan brought together national and local leaders in Pennsylvania to exchange ideas, share successes and discuss solutions to the opioid epidemic in our communities. The free, second-annual conference featured keynote addresses and workshops and highlighted the proactive efforts of local organizations. Participants included national and state officials, county human services and drug and alcohol leaders, legislative staff, providers and community stakeholders.
Not staying silent on the silent epidemic
Magellan is actively helping individuals and families on their path to recovery. Further, to educate the public, doctors and other healthcare providers, we offer resources on our Magellan Health OPIOID INSIGHTS microsite. The site includes links to blog posts, videos, resources and published articles.
Hosting a forum for sharing successes and discussing solutions
InSeptember2018, Magellan brought together national and local leaders in Pennsylvania to exchange ideas, share successes and discuss solutions around the challenge we face together in addressing the opioid epidemic in our communities. The second-annual conference featured keynote addresses and workshops and highlighted the proactive efforts of local organizations. Participants at the free one-and-a-half-day conference included national and state officials, county human services and drug and alcohol leaders, legislative staff, providers and community stakeholders.
 Dr. Shareh Ghani, vice president medical director at Magellan Healthcare, and lead author of the study spoke of the importance of fully understanding the scope of the addiction crisis: “Having worked in commercial and Medicaid markets, I have reviewed numerous cases of accidental overdose and suicides related to pain prescriptions. The opioid crisis in this country demands that we understand the issue and identify predictors of risk.”
Dr. Shareh Ghani, vice president medical director at Magellan Healthcare, and lead author of the study spoke of the importance of fully understanding the scope of the addiction crisis: “Having worked in commercial and Medicaid markets, I have reviewed numerous cases of accidental overdose and suicides related to pain prescriptions. The opioid crisis in this country demands that we understand the issue and identify predictors of risk.”